Silicone oil internal tamponade has been used for over 50 years, even prior to pars plana vitrectomy [1].Over a course of time silicone oil may migrate to the anterior chamber through the pupil. This may disperse in the form of small globules or emulcify into finer droplets [2] leading to obstruction of the angles or the trabecular meshwork leading to glaucoma. I present a case where a single large oil globule initially presented as pupil block glaucoma which later remains in the pupillary area causing a myopic refractive error.
Case report
A 58-year-old man presented with a unilateral white cataract with only light perception. His vision had been declining over a year. On questioning about trauma, he gave an insignificant history of a shuttlecock injury about 20 years previously. He did not have any symptoms until the vision reduced from increasing cataract. Preoperative assessment showed good pupillary reaction, good light projection and positive Maddox rod test for macular function. B’scan ultrasonography did not reveal any evidence of retinal detachment and the vitreous was clear. He had a planned extracapsular cataract extraction and a +19.0 Dioptre one piece posterior chamber implant was inserted in the sulcus for emmetropic correction. There were no intraoperative complications.
On first postoperative day unaided visual acuity was 6/60 at best with no further improvement with pinhole. He was found to have an inferior half chronic shallow detachment with inferior dialysis extending from 5-7 o’clock. He was referred to the local retinal surgeon who treated him promptly with pars-plana vitrectomy with silicone oil tamponade.
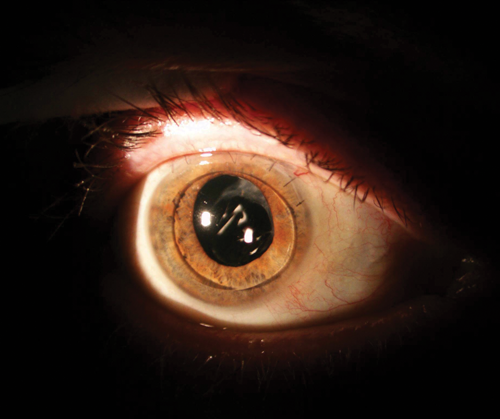
Figure 1.
One week after the operation the patient presented to a sister hospital with severe pain and was found to have pupil block glaucoma with intraocular pressure (IOP) in excess of 60mmHg. He was treated with pupil dilatation, Diamox and pressure reducing drops. Over the next two weeks the IOP improved to 18mmHg, the eye was comfortable and we were able to stop the Diamox. There was a single silicone oil bubble in the form of a biconvex lens in front of the pupil and covering it (Figure 1). For the untrained eye this would have looked like an anterior chamber implant with pupil capture. The anterior chamber (AC) remained deep, the iris plane flat and there were no other silicone bubbles in the AC or the angles. Fundus view was difficult but the retina was found to be flat. The unaided acuity was counting fingers. Refraction was -6.00/-1.50x180. The cylinder was probably due to the corneal astigmatism but the high myopic refraction was thought to be due to the hypermetropic effect of the silicone oil lenticule. A corrected visual acuity of 6/36 was obtained.
Discussion
Following silicone oil internal tamponade, the oil finds its way into the AC over a short or long period of time. This may be in the form of dispersion comprising larger globules or multiple much finer bubbles due to emulcification [2]. Other mechanisms are, overfill with silicone oil where the oil fills the AC fully or causing anterior displacement of the iris diaphragm causing angle closure glaucoma and inflammation exacerbating pre-existing glaucoma [3].
In this patient, a large single bubble initially obstructed the pupil causing pupil block glaucoma and later coming to lie in front of the pupil causing a refractive error. Continuous aqueous formation tends to raise the silicone oil which is of lighter specific gravity into the pupil pathway, as shown by Lilly Zborowski-Gutman et al. [4].The availability of heavy silicone oil may change this pattern and and as a result pupil block glaucoma may occur less frequently. Patients with pupil block glaucoma should be managed by dilating the pupil, YAG laser peripheral iridotomy if appropriate, reducing aqueous production by using Diamox and pressure reducing drops in any combination, notably betablockers or alpha agonists. In the case of oil dispersion or emulcification, treatment may be necessary if the IOP is elevated. Long-term effects of silicone oil in the AC include corneal toxicity and decompensation [5]. Therefore when the retinal surgeon decides to drain the oil, he or she may also do an anterior chamber washout or may leave this to the anterior segment surgeon. This case illustrates an additional indication for the removal of silicone oil for refractive reasons.
References
1. Cibis PA, Becker B, Okun E, Canaan S. The use of silicon oil in retinal detachment surgery. Arch Ophthalmol 1962;681:590-9.
2. Patel AV, Papakostas TD, Eliott D. Silicone oil emulcification in retina surgery. Retina Today September 2015;29-32.
3. Ichhpujani P, Jindal A, Jay Katz L. Silicone oil induced glaucoma: a review. Graefes Arch Clin Exp Ophthalmol 2009;247:1585-93.
4. Lilly Zborowski-Gutman, G Treister, N Naveh, et al. Acute glaucoma following vitrectomy and silicon oil injection. Brit J Ophthalmol 1987;71:903-6.
5. Gurwood AS. Her vision is on the bubble. Review of Optometry website. January 2015.
COMMENTS ARE WELCOME



